State 17213 Form in PDF
State 17213 Form in PDF
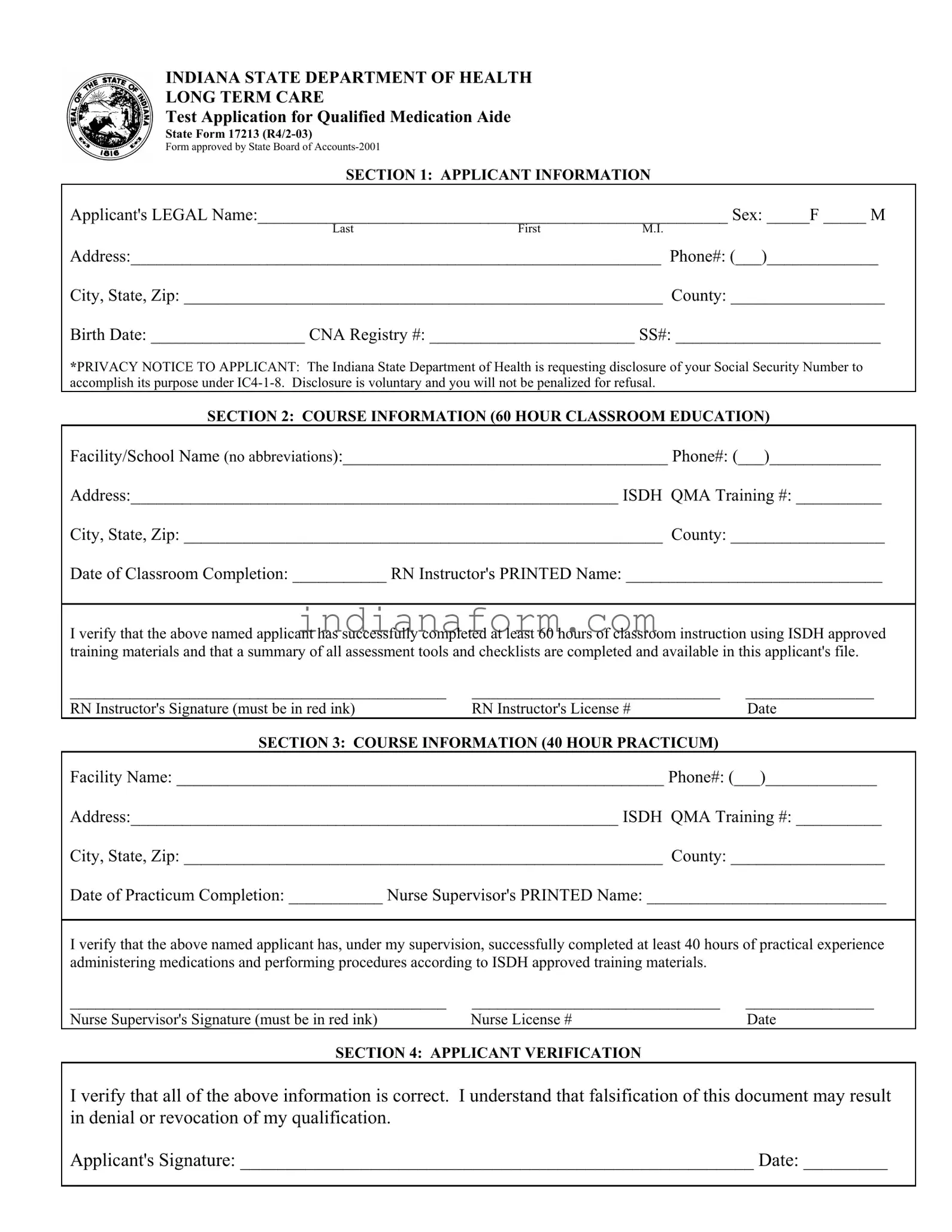
In the realm of healthcare, particularly within the state of Indiana, the State Form 17213 stands as a critical document for individuals aspiring to become Qualified Medication Aides (QMA). Authored by the Indiana State Department of Health and adhering to the standards laid out by the State Board of Accounts in 2001, this form delineates the application process involved in attaining certification. As outlined, the application encompasses a comprehensive approach beginning with the collection of applicant's personal information, including a unique stipulation regarding the voluntary disclosure of Social Security Numbers under specific legislative authority. Integral to the certification journey, the form requires detailed accounting of both theoretical and practical training components—a 60-hour classroom education followed by a 40-hour practicum, each verified by qualified professionals. Furthermore, it highlights the necessity of honest self-verification by the applicants concerning the accuracy of the information provided, underscoring the serious implications of falsification. The document also elaborates on various candidate statuses, accommodating a broader spectrum of applicants, such as out-of-state QMAs and nursing students. Finally, it concludes with procedural guidelines for the submission of necessary documentation and the testing fee, setting the stage for the examination process. Through this form, Indiana meticulously structures the pathway for aspiring medication aides, ensuring a standard of competency and care is upheld in the long-term healthcare landscape.
INDIANA STATE DEPARTMENT OF HEALTH
LONG TERM CARE
Test Application for Qualified Medication Aide
State Form 17213
Form approved by State Board of
SECTION 1: APPLICANT INFORMATION
Applicant's LEGAL Name:_______________________________________________________ Sex: _____F _____ M
LastFirstM.I.
Address:______________________________________________________________ Phone#: (___)_____________
City, State, Zip: ________________________________________________________ County: __________________
Birth Date: __________________ CNA Registry #: ________________________ SS#: ________________________
*PRIVACY NOTICE TO APPLICANT: The Indiana State Department of Health is requesting disclosure of your Social Security Number to accomplish its purpose under
SECTION 2: COURSE INFORMATION (60 HOUR CLASSROOM EDUCATION)
Facility/School Name (no abbreviations):______________________________________ Phone#: (___)_____________
Address:_________________________________________________________ ISDH QMA Training #: __________
City, State, Zip: ________________________________________________________ County: __________________
Date of Classroom Completion: ___________ RN Instructor's PRINTED Name: ______________________________
I verify that the above named applicant has successfully completed at least 60 hours of classroom instruction using ISDH approved training materials and that a summary of all assessment tools and checklists are completed and available in this applicant's file.
____________________________________________ |
_____________________________ |
_______________ |
RN Instructor's Signature (must be in red ink) |
RN Instructor's License # |
Date |
SECTION 3: COURSE INFORMATION (40 HOUR PRACTICUM)
Facility Name: _________________________________________________________ Phone#: (___)_____________
Address:_________________________________________________________ ISDH QMA Training #: __________
City, State, Zip: ________________________________________________________ County: __________________
Date of Practicum Completion: ___________ Nurse Supervisor's PRINTED Name: ____________________________
I verify that the above named applicant has, under my supervision, successfully completed at least 40 hours of practical experience administering medications and performing procedures according to ISDH approved training materials.
____________________________________________ |
_____________________________ |
_______________ |
Nurse Supervisor's Signature (must be in red ink) |
Nurse License # |
Date |
SECTION 4: APPLICANT VERIFICATION
I verify that all of the above information is correct. I understand that falsification of this document may result in denial or revocation of my qualification.
Applicant's Signature: _______________________________________________________ Date: _________
SECTION 5: CANDIDATE STATUS
□ 100 HOUR CLASS |
□ |
□ Psychiatric Attendant |
□ Nursing Student - School: ______________________________________ |
□ Other: _________________________ |
□ Foreign Nurse - Country: ______________________________________ |
|
|
|
SECTION 6: DOCUMENTATION |
The following required documents are included with this request to test: |
|
□ Original Application |
□ Copy of High School Diploma, GED or transcript |
□ Original documentation of practicum |
□ Copy of current Indiana Nurse Aide Registry certification letter |
Nursing Students and
□ Original ISDH approval letter & all documentation initially submitted to ISDH
Include testing fee of $60.00 (money order) payable to Professional Resources. Personal checks are not accepted. Send all documentation and fee to: Professional Resources, PO Box 1552, Valparaiso, IN
FIRST TESTING |
SECTION 7: TEST RESULTS |
Test Entity |
|
Tester
Test Date
Test Site
County
WRITTEN TEST RESULTS: |
PASS ______ |
FAIL _______ |
SCORE:_______
SECOND TESTING
Test Entity
Tester
Test Site
Test Date
County
WRITTEN TEST RESULTS: |
PASS ______ |
FAIL _______ |
SCORE:_______
THIRD TESTING
Test Entity
Tester |
|
|
Test Date |
|
|
|
|
Test Site |
|
|
County |
|
|
|
|
WRITTEN TEST RESULTS: |
PASS ______ |
FAIL _______ |
SCORE:_______ |
|
|
|
|
| Fact | Detail |
|---|---|
| 1. Form Identification | Indiana State Department of Health Long Term Care Test Application for Qualified Medication Aide, State Form 17213 (R4/2-03) |
| 2. Approving Authority | Form approved by State Board of Accounts-2001 |
| 3. Purpose | To apply for the Qualified Medication Aide Test in Indiana |
| 4. Training Requirement | At least 60 hours of classroom education plus 40 hours of practicum |
| 5. Instructor Verification | Verification by the RN Instructor and Nurse Supervisor is required, with signatures in red ink |
| 6. Applicant Verification | The applicant must verify the information provided is correct and understands falsification may result in denial or revocation of qualification |
| 7. Privacy Notice | Disclosing Social Security Number is voluntary under IC4-1-8, with no penalty for refusal |
| 8. Additional Candidate Status | Candidates can apply as a 100 Hour Class, Out-of-State QMA, Psychiatric Attendant, Nursing Student, or Foreign Nurse |
| 9. Documentation Required | Includes original application, proof of education, documentation of practicum, and Indiana Nurse Aide Registry certification letter. Nursing Students and Out-of-State QMAs must also include ISDH approval letter & documentation submitted to ISDH |
| 10. Testing Fee and Submission | A $60.00 money order payable to Professional Resources, with no personal checks accepted. Documentation and fee sent to Professional Resources, PO Box 1552, Valparaiso, IN 46384-1552 |
After ensuring eligibility and gathering the necessary documentation, the next step is to fill out the State 172(figures omitted) form carefully. This step is crucial in applying for the Qualified Medication Aide Test in Indiana. Accuracy and completeness are essential to avoid delays or rejection. Following the outlined steps will help streamline the process.
Completing the State 17213 form accurately and providing all required documentation are significant steps in the application process for the Qualified Medication Aide Test. It is important for applicants to thoroughly review their application before submission to ensure all information is correct and complete. This diligence will help ensure a smooth and efficient processing experience.
What is the purpose of the State Form 17213?
State Form 17213, issued by the Indiana State Department of Health, serves as the Test Application for Qualified Medication Aide (QMA) certification. Its primary purpose is to facilitate the application process for individuals seeking to become certified as Qualified Medication Aides in Indiana. By completing this form, applicants are taking the first step towards certification, which involves verifying their completion of the requisite training programs and eligibility to sit for the certification examination.
Who needs to complete the State Form 17213?
This form must be completed by individuals who have successfully finished the required classroom and practicum training to become a Qualified Medication Aide in Indiana and are ready to take the certification test. The form is applicable to a wide range of candidates, including but not limited to, current nursing students, psychiatric attendants, out-of-state Qualified Medication Aides seeking certification in Indiana, and foreign-trained nurses.
What are the required documents to be submitted along with State Form 17213?
Along with the completed application form, candidates must submit several documents as part of their application package. These include the original application form, a copy of their high school diploma, GED, or transcript, original documentation of their practicum completion, and a copy of their current Indiana Nurse Aide Registry certification letter. Candidates who are nursing students or out-of-state Qualified Medication Aides must also include an original Indiana State Department of Health approval letter and all documentation that was initially submitted to ISDH. It's important to note that a testing fee of $60, payable via money order to Professional Resources, is also required. Personal checks are not accepted.
How is the testing fee for the State Form 17213 certification test paid?
The testing fee, which amounts to $60, must be paid through a money order made payable to Professional Resources. The form, along with the necessary documentation and the testing fee, should be sent to Professional Resources at the specified address. It's crucial to remember that personal checks are not accepted for the payment of this fee.
What happens after submitting the State Form 17213?
After submitting the State Form 17213 along with all the required documentation and the testing fee, candidates are scheduled for the certification test. The test results are provided in three sections: first testing, second testing, and third testing, if applicable. Each section documents the test entity, tester, test site, test date, county, and the candidates' results — indicating whether they passed or failed, along with their scores.
Can someone be penalized for not providing their Social Security Number on the State Form 17213?
No, applicants are not penalized for withholding their Social Security Number on the State Form 17213. The Indiana State Department of Health requests the disclosure of an applicant’s Social Security Number under IC4-1-8 for identification purposes. However, disclosure is voluntary, and applicants have the right to refuse without facing any penalties.
Filling out State Form 17213, required for a Qualified Medication Aide (QMA) certification in Indiana, demands careful attention to detail. Common mistakes can lead to processing delays or even the denial of certification. It's beneficial for applicants to be mindful of these pitfalls to ensure a smooth application process.
The first frequent error occurs in Section 1, where applicants must provide their legal name. Often, individuals may unintentionally use nicknames or abbreviations, which can lead to verification issues, as this information must match other legal documents precisely.
In Section 2, regarding course information, a common mistake is not providing the full name of the facility or school where the classroom education took place. Abbreviations or informal names can complicate the verification process, thereby hindering the application. Moreover, the diligent verification of the RN instructor's signature in red ink is crucial. This specific requirement, if overlooked, can invalidate the section.
Another slip-up takes place in Section 3, where details of the practicum are documented. The nurse supervisor's license number and signature in red ink are often incorrectly provided or entirely missed. This documentation is vital for confirming the practical experience component of the certification.
Section 4's verification by the applicant is a step frequently bypassed. Applicants must understand that this section's accuracy is paramount and falsification can lead to serious consequences, including denial or revocation of the qualification.
Section 5, which outlines the candidate status, is another area where errors are common. Failure to accurately indicate the applicable status, such as out-of-state QMA or nursing student, can mislead the reviewing department, leading to unnecessary back-and-forth and potential rejection.
Including all necessary documentation as listed in Section 6 is crucial. Applicants often forget one or more of the following required documents:
Last but not least, applicants often neglect to send the complete package to the correct address, as specified. This may seem trivial, but incorrect or incomplete addresses can lead to lost applications or further delays. Ensuring the completeness and accuracy of the application package is essential for a successful certification process.
Being mindful of these common mistakes and adhering closely to the form's requirements will greatly assist applicants in achieving their goal of becoming a certified Qualified Medication Aide.
When completing the State Form 17213 for the Indiana State Department of Health's Long Term Care Test Application for Qualified Medication Aide, it is essential to have all necessary documents prepared and organized. This ensures a smoother application process, enhancing the chances for approval. Below is a list of other forms and documents often used alongside the State 17213 form, each serving a critical role in the completion and submission process.
Gathering and preparing these documents along with the State Form 17213 is vital for a successful application and testing process. Applicants are reminded to review their application packet thoroughly to ensure completeness and accuracy before submission. This careful preparation can lead to a more straightforward and less stressful certification journey.
The State 17213 form is similar to other documents used in the healthcare and education sectors for certification or verification purposes. Each document, while serving a unique function, shares common elements with the State 17213 form, such as the collection of personal information, the requirement for educational prerequisites, and the need for verification from licensed professionals.
National Council Licensure Examination (NCLEX) Application: Just like the State 17213 form, the NCLEX application gathers extensive applicant information, including educational background and personal details. Both forms serve as a gateway to professional certification within the healthcare field, albeit for different roles. The NCLEX application is focused on nurses seeking licensure to practice, emphasizing the need for completion of nursing education and passing a standardized examination. Similarly, the State 11213 form requires completion of specialized education and practical experience, particularly for those aiming to become Qualified Medication Aides.
Certified Nursing Assistant (CNA) Certification Renewal Form: This form shares similarities with the State 17213, especially in the sections that require proof of continued education and practical experience. CNAs must often submit documentation of ongoing professional development, just as applicants of the State 17213 form must provide evidence of completed classroom and practical training. Both documents underscore the importance of maintaining competent practice in healthcare settings, ensuring that individuals are up-to-date with their skills and knowledge.
Application for Professional Rescertification: Many professions within healthcare require periodic recertification to ensure that professionals remain qualified to practice, reflecting a principle similar to the State 17213 form's purpose. These applications often require the applicant to list recent educational courses or seminars attended, much like the section on the State 17213 form that details course information and practicum completion. Additionally, both types of documents frequently incorporate sections for the verification of the applicant's information by a supervising professional, ensuring that all stated qualifications are legitimate and current.
When filling out the State Form 17213 for the Indiana State Department of Health, there are several important steps and precautions to keep in mind. Here are some do's and don'ts to ensure the process goes smoothly:
Do's:By following these do's and don'ts, you can complete the State Form 17213 effectively, ensuring a smoother process for your qualified medication aide test application.
Understanding the State 17213 Form, a crucial application in Indiana for those aspiring to become Qualified Medication Aides, is vital. Several misconceptions surround this form, leading to confusion and errors in application. To clarify, below are ten common misconceptions about the State 17213 form:
Understanding these misconceptions is the first step towards a successful application process. Applicants are encouraged to read the details of the State 17213 form carefully and to seek clarification when necessary to ensure a smooth path to becoming a Qualified Medication Aide.
Filling out the State 17213 form is an important step for becoming a Qualified Medication Aide (QMA) in Indiana. To ensure the process is smooth and compliant, here are some key takeaways to keep in mind:
By closely following these guidelines, applicants can navigate the process of completing and submitting the State 17213 form more efficiently, bringing them one step closer to becoming a Qualified Medication Aide in Indiana.
State 41769 - Ensures that every action taken under the permit, particularly alterations or repairs, follows guidelines to avoid damage to state property.
Indiana Tax Forms - Used by individuals or companies to provide financial assurance to the Indiana Department of Transportation for permitted projects.
Uc-5a - Completing the UC 5A accurately helps streamline the unemployment benefits process for displaced workers.