State 28808 Form in PDF
State 28808 Form in PDF
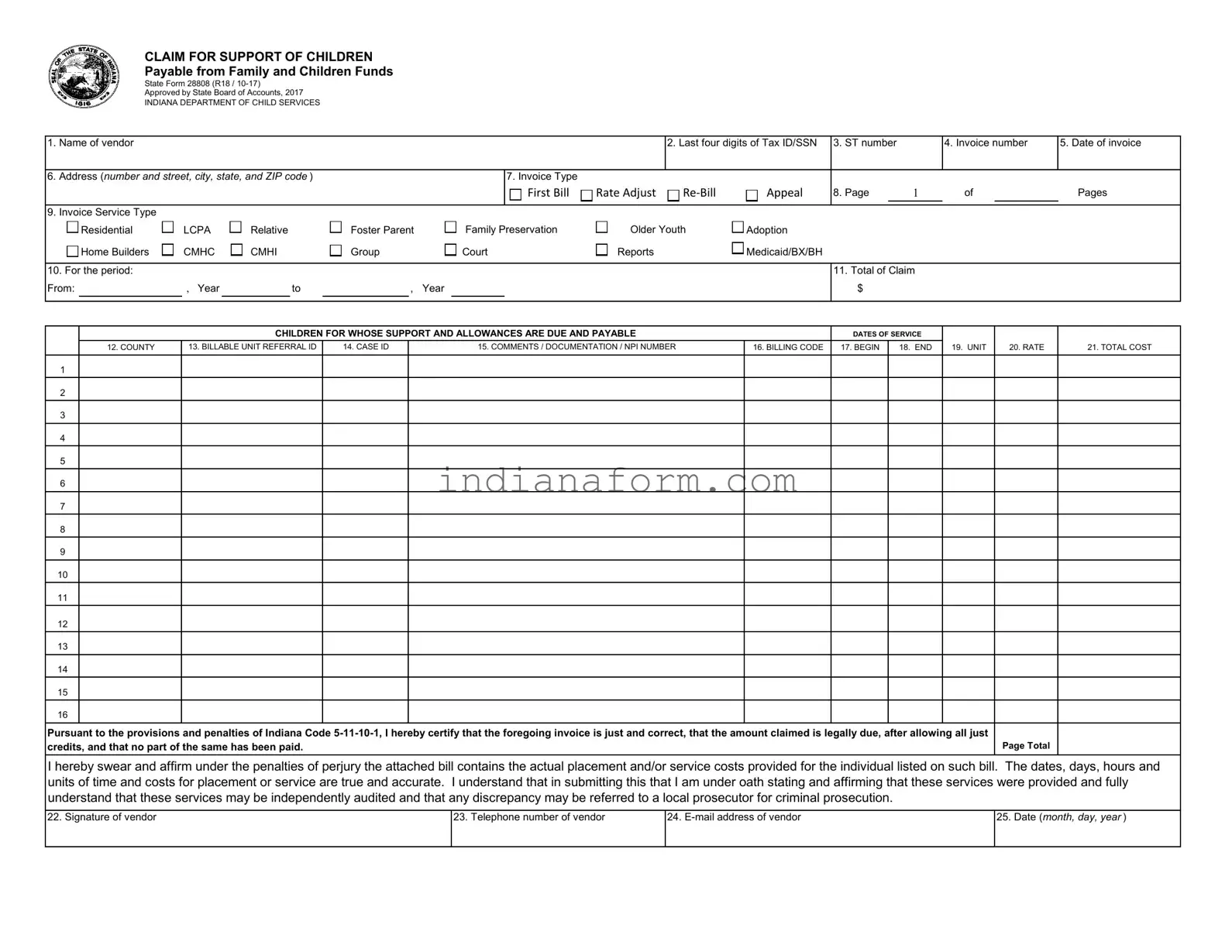
The heart of the financial support system for children under state care in Indiana is meticulously detailed in the State Form 28808, a document that epitomizes the structured approach to ensuring children's welfare through regulated financial channels. Approved by the State Board of Accounts in 2017 and operating under the auspices of the Indiana Department of Child Services, this form serves a critical function in the disbursement of funds from Family and Children Funds, designated for the upkeep, support, and service provisions for children. Vendors, ranging from foster care providers to various service-oriented entities, are required to submit this form, which captures essential information including the vendor’s details, service types, and financial claims for specified periods. Encompassing a wide array of services such as residential placement, family preservation, and adoption support, the form requires meticulous documentation of service dates, rates, and total costs associated with the care provided. Furthermore, it mandates adherence to legal and ethical standards by requiring the vendor’s certification of the accuracy and legality of the claim under penalty of perjury, thereby reinforcing the accountability framework within which child support services operate in the state. Through its comprehensive design, the State Form 28808 not only streamlines the process of financial claims for child support but also embeds a layer of audit and verification to protect against misuse, ensuring that the provision of services to children in need is both efficient and transparent.
CLAIM FOR SUPPORT OF CHILDREN
Payable from Family and Children Funds
State Form 28808 (R18 /
Approved by State Board of Accounts, 2017
INDIANA DEPARTMENT OF CHILD SERVICES
1. |
Name of vendor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last four digits of Tax ID/SSN |
3. ST number |
|
4. Invoice number |
5. Date of invoice |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. |
Address (number and street, city, state, and ZIP code ) |
|
|
|
|
|
|
|
7. Invoice Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Bill |
|
|
Rate Adjust |
|
|
Appeal |
8. Page |
1 |
of |
|
Pages |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Invoice Service Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Residential |
|
|
LCPA |
|
|
|
Relative |
|
|
Foster Parent |
|
|
Family Preservation |
|
|
|
Older Youth |
|
|
Adoption |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
Home Builders |
|
|
CMHC |
|
|
|
CMHI |
|
|
Group |
|
|
Court |
|
|
|
Reports |
|
|
Medicaid/BX/BH |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. For the period: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Total of Claim |
|
|
|
|||||||
From: |
|
, Year |
|
|
|
|
to |
|
|
|
, Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
CHILDREN FOR WHOSE SUPPORT AND ALLOWANCES ARE DUE AND PAYABLE |
|
|
DATES OF SERVICE |
|
|
|
||||||||||||||||||||||
|
|
|
12. COUNTY |
13. BILLABLE UNIT REFERRAL ID |
|
|
14. CASE ID |
|
15. COMMENTS / DOCUMENTATION / NPI NUMBER |
16. BILLING CODE |
17. BEGIN |
18. END |
19. UNIT |
20. RATE |
21. TOTAL COST |
|||||||||||||||||||||||
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
Pursuant to the provisions and penalties of Indiana Code |
Page Total |
credits, and that no part of the same has been paid. |
I hereby swear and affirm under the penalties of perjury the attached bill contains the actual placement and/or service costs provided for the individual listed on such bill. The dates, days, hours and units of time and costs for placement or service are true and accurate. I understand that in submitting this that I am under oath stating and affirming that these services were provided and fully understand that these services may be independently audited and that any discrepancy may be referred to a local prosecutor for criminal prosecution.
22. Signature of vendor
23. Telephone number of vendor
24.
25.Date (month, day, year )
CLAIM FOR SUPPORT OF CHILDREN
Payable from Family and Children Funds
State Form 28808 (R18 /
Approved by State Board of Accounts, 2017
INDIANA DEPARTMENT OF CHILD SERVICES
1. |
Name of vendor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last four digits of Tax ID/SSN |
3. ST number |
|
4. Invoice number |
5. Date of invoice |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. |
Address (number and street, city, state, and ZIP code ) |
|
|
|
|
|
|
|
7. Invoice Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Bill |
|
|
Rate Adjust |
|
|
|
|
Appeal |
8. Page |
1 |
of |
|
Pages |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Invoice Service Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Residential |
|
|
LCPA |
|
|
|
Relative |
|
|
Foster Parent |
|
|
Family Preservation |
|
Older Youth |
|
|
Adoption |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
Home Builders |
|
|
CMHC |
|
|
|
CMHI |
|
|
Group |
|
|
Court |
|
Reports |
|
|
Medicaid/BX/BH |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. For the period: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Total of Claim |
|
|
|
|||||||
From: |
|
, Year |
|
|
|
|
to |
|
|
|
, Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
CHILDREN FOR WHOSE SUPPORT AND ALLOWANCES ARE DUE AND PAYABLE |
|
|
|
|
DATES OF SERVICE |
|
|
|
||||||||||||||||||||
|
|
|
12. COUNTY |
13. BILLABLE UNIT REFERRAL ID |
|
|
14. CASE ID |
|
15. COMMENTS / DOCUMENTATION / NPI NUMBER |
|
|
16. BILLING CODE |
17. BEGIN |
18. END |
19. UNIT |
20. RATE |
21. TOTAL COST |
|||||||||||||||||||||
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
Pursuant to the provisions and penalties of Indiana Code |
Page Total |
credits, and that no part of the same has been paid. |
I hereby swear and affirm under the penalties of perjury the attached bill contains the actual placement and/or service costs provided for the individual listed on such bill. The dates, days, hours and units of time and costs for placement or service are true and accurate. I understand that in submitting this that I am under oath stating and affirming that these services were provided and fully understand that these services may be independently audited and that any discrepancy may be referred to a local prosecutor for criminal prosecution.
22. Signature of vendor
23. Telephone number of vendor
24.
25.Date (month, day, year )
CLAIM FOR SUPPORT OF CHILDREN
Payable from Family and Children Funds
State Form 28808 (R18 /
Approved by State Board of Accounts, 2017
INDIANA DEPARTMENT OF CHILD SERVICES
1. |
Name of vendor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last four digits of Tax ID/SSN |
3. ST number |
|
4. Invoice number |
5. Date of invoice |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. |
Address (number and street, city, state, and ZIP code ) |
|
|
|
|
|
|
|
7. Invoice Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Bill |
|
|
Rate Adjust |
|
|
|
|
Appeal |
8. Page |
1 |
of |
|
Pages |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Invoice Service Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Residential |
|
|
LCPA |
|
|
|
Relative |
|
|
Foster Parent |
|
|
Family Preservation |
|
Older Youth |
|
|
Adoption |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
Home Builders |
|
|
CMHC |
|
|
|
CMHI |
|
|
Group |
|
|
Court |
|
Reports |
|
|
Medicaid/BX/BH |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. For the period: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Total of Claim |
|
|
|
|||||||
From: |
|
, Year |
|
|
|
|
to |
|
|
|
, Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
CHILDREN FOR WHOSE SUPPORT AND ALLOWANCES ARE DUE AND PAYABLE |
|
|
|
|
DATES OF SERVICE |
|
|
|
||||||||||||||||||||
|
|
|
12. COUNTY |
13. BILLABLE UNIT REFERRAL ID |
|
|
14. CASE ID |
|
15. COMMENTS / DOCUMENTATION / NPI NUMBER |
|
|
16. BILLING CODE |
17. BEGIN |
18. END |
19. UNIT |
20. RATE |
21. TOTAL COST |
|||||||||||||||||||||
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
Pursuant to the provisions and penalties of Indiana Code |
Page Total |
credits, and that no part of the same has been paid. |
I hereby swear and affirm under the penalties of perjury the attached bill contains the actual placement and/or service costs provided for the individual listed on such bill. The dates, days, hours and units of time and costs for placement or service are true and accurate. I understand that in submitting this that I am under oath stating and affirming that these services were provided and fully understand that these services may be independently audited and that any discrepancy may be referred to a local prosecutor for criminal prosecution.
22. Signature of vendor
23. Telephone number of vendor
24.
25.Date (month, day, year )
INSTRUCTIONS FOR COMPLETING A CLAIM FOR SUPPORT OF CHILDREN
October 2017
*= Required field.
1.*NAME – Legal name of benefit/product/service provider; must match name submitted via the Vendor Information Form.
2.*LAST FOUR DIGITS OF TAX ID – The last four digits of the Federal Tax Identification Number associated with the legal name in Section 1. This is your Social Security Number for individuals (e.g.foster parents).
3.*ST NUMBER – State Vendor ID # assigned by the DCS payment system (KidTraks). This 6 digit number can be found on the Warrant Summary.
ST Numbers are also available at https://magik.dcs.in.gov/Portal/Home/Login?ReturnUrl=%2fportal%2f. From there, select "Provider Service Guide" and enter your Tax ID in the appropriate space provided.
4.*INVOICE NUMBER – assigned by the vendor; CAN BE NO LONGER THAN 8 CHARACTERS; should be a unique number for each submission and can include letters and/or numbers (e.g. "Nov2010" or "1001").
5.*DATE OF INVOICE – Date assigned by the vendor as the date of the claim. Invoices must be received by DCS KidTraks Invoicing within 10 business days of this date.
6.*ADDRESS – Vendor's complete address, which should match the most recent Vendor Information form on file.
7.*INVOICE TYPE – Is the invoice being submitted the first submission, a rate adjustment, a
8.*PAGE NUMBER – Includes the current page number as well as the total number of pages included in the Claim (limited to a total of 3 pages per Invoice).
9.*INVOICE SERVICE TYPE – Only one overriding service type should be picked for all sevice codes being invoice in column 16. The invoice service type should reflect all services being invoiced.
10.*FOR THE PERIOD – The beginning and end dates of the month being billed on the Claim. (e.g. January services would be: From January 1, 2011 to January 31, 2011).
The Claim period should not be confused with the Dates of Service (Sections 17 and 18) as vendors may list multiple children/Case #s/Referral IDs with different dates of service during the Claim period.
11.*TOTAL OF CLAIM – The cumulative sum of the Total Cost columns (col. 21) of all invoice pages
This total cannot be adjusted upward once it's been submitted.
12.*COUNTY – Name of County that authorized services to be rendered for the child being served. For Post Adoption or Independent Living services, please enter County of child’s residence. NOTE: An invoice can include line items for multiple counties.
13.*BILLABLE UNIT REFERRAL ID– Billable Unit Referral ID (PL# or RF#) for Service Referrals; Probation will still use Case number until fully implemented on the Referral Wizard.
14.*CASE ID – This is the case number in KidTraks and is required for all foster care invoices as well as all provider invoices for all services.
15.*COMMENTS / DOCUMENTATION / NPI NUMBER – Spaces can also be used to provide explanation / documentation to support payments and NPI number of doctor.
16.*BILLING CODE – Includes both Service and Component Codes for the benefit/product/service provided. Provider codes are available at https://magik.dcs.in.gov/Portal/Home/Login?ReturnUrl=%2fportal%2f From there, select "Provider Service Guide" and enter your Tax ID or DCS Vendor ID (i.e. ST Number) in the appropriate space provided.
17.*BEGIN DATE OF SERVICE – First day the benefit/product/service was provided. If the service was provided in one day, the Begin Date and End Dates will be the same.
18.*END OF DATE OF SERVICE – Last day the benefit/product/service was provided. If the service was provided in one day, the Begin Date and End Dates will be the same.
19.*UNIT – The number of times a benefit/product/service was rendered during the Claim period.
Units are defined in contracts/agreements and are typically
20.*RATE – The amount
21.*TOTAL COST – The total amount of the line item calculated by multiplying the number of units by the rate (Unit x Rate=Total Cost)
22.*SIGNATURE OF VENDOR – Authorizing signature of vendor submitting the Claim. All pages submitted must be signed; blue ink is strongly recommended.
23.* TELEPHONE NUMBER OF VENDOR – Telephone number for Vendor, to be used only for clarifications and resolution of billing issues.
24.
25.*DATE – This is the date the invoice was completed/signed. This date can not be before the last day of service.
| Fact | Description |
|---|---|
| Form Identification | State Form 28808 (R18 / 10-17) |
| Purpose | Claim for Support of Children Payable from Family and Children Funds |
| Approval | Approved by State Board of Accounts, 2017 |
| Applicable Law | Indiana Code 5-11-10-1 |
| Governing Body | Indiana Department of Child Services |
| Key Elements on Form | Vendor information, invoice details, service type, period of claim, amount claimed, service dates, and payment certification |
Filling out State Form 28808, also known as the Claim for Support of Children Payable from Family and Children Funds, is an important process for vendors providing services to children under the Indiana Department of Child Services umbrella. This form ensures that vendors receive compensation for their invaluable services. The steps below guide you through filling out this form accurately, thereby facilitating a smoother transaction with the Indiana Department of Child Services.
Upon completing this form with the necessary details and reviewing for accuracy, you ensure prompt and correct payment for services rendered. The thoroughness and accuracy of your completion are imperative for a seamless process with the Indiana Department of Child Services, ultimately supporting the welfare and support of the children in the program.
What is the purpose of the State 28808 form?
The State 28808 form is used for submitting a claim for child support payments payable from Family and Children Funds in Indiana. The form ensures that children’s support and allowances are duly processed and paid by documenting the services provided and the associated costs.
Who is required to complete this form?
Any vendor authorized to provide services to children under the supervision of the Indiana Department of Child Services must complete this form. This includes residential care providers, foster parents, adoption services, and other child welfare-related service providers.
What information do I need to complete State Form 28808?
Completing the form requires information including the vendor's name, Tax ID, State Vendor ID, invoice number, date of invoice, and address. Details on the invoice type, service type, period of claim, children's information, services provided, and the cost of these services are also necessary. Additionally, the form requires the vendor's signature, telephone number, and email address.
How do I submit State Form 28808?
After accurately filling out the form, ensure every page is signed (preferably in blue ink) and submit it to the designated office within the Indiana Department of Child Services. It must be submitted within 10 business days of the invoice date.
Can I adjust the Total of Claim after submission?
No, once the Total of Claim has been submitted, it cannot be adjusted upward. Ensure all calculations are correct before submission to avoid discrepancies and potential delays.
What happens if there is a discrepancy in the submitted invoice?
Invoices are subject to independent audits. Should any discrepancy arise, the case may be referred to a local prosecutor for criminal prosecution. It is crucial to ensure that all information provided on the form is accurate and truthful.
Why is it recommended to sign the form in blue ink?
Signing in blue ink helps distinguish the original document from photocopies or digital copies, ensuring the authenticity and integrity of the form when it is reviewed by the Indiana Department of Child Services.
Filling out the State Form 28808, particularly for claims from the Family and Children Funds, demands attention to detail. Frequently, errors occur that can delay processing or result in denied claims. Understanding these common pitfalls can streamline the submission process.
Several mistakes are commonly made:
Common areas overlooked also include:
Ensuring accuracy in these fields is paramount. Missteps not only cause processing delays but can also lead to denied claims or the necessity for re-submission, each of which carries its own set of frustrations and delays. Diligence and careful review of the claim form prior to submission will significantly mitigate these risks and contribute to a smoother claims process.
When dealing with State Form 28808 in the context of child support claims in Indiana, various other forms and documents tend to be necessary for a comprehensive approach to child support and welfare cases. These additional documents ensure accurate and timely processing of claims, along with adherence to legal and procedural requirements. They span a range of purposes, from establishing paternity to appealing decisions regarding child support.
Together, these forms and documents support the primary function of State Form 28808 by providing a full circle of documentation needed for the establishment, enforcement, modification, and, eventually, the termination of child support. They serve to protect the interests of the child while ensuring fairness to the parents or guardians involved. Accurate completion and timely submission of these forms are crucial for the effective functioning of child support services.
The State 28808 form is similar to several other legal documents used within the context of child welfare and support services. Each of these documents serves a specific purpose, yet they share common characteristics with the State 28808 form, such as providing detailed information on services rendered, cost calculations, and identification of service providers and recipients.
The Financial Statement for Child Support is a document often used in family law to detail the financial obligations of a parent toward their child. Like the State 28808 form, it requires detailed financial information, including income sources, expenditures related to the child's care, and other relevant financial data. Both forms are integral in calculating the financial responsibilities of parents and ensuring the well-being of children through financial support.
The Child Welfare Agency Service Invoice shares similarities with the State 28808 form in its function of billing for child-related services. It typically includes details such as the service provider's information, services rendered, period of service, and costs. Both documents are used by agencies to claim expenses incurred while providing care or services to children, whether through foster care, adoption, or family preservation efforts.
The Foster Care Placement Agreement is a contract between a foster care agency and a foster parent, detailing the responsibilities of both parties in the care of a foster child. While this document focuses more on the terms of care rather than financial aspects, it often includes sections on reimbursement or support similar to the information found in the State 28808 form, such as rates and billing codes for foster care services.
When completing the State 28808 form for claiming support of children, it is essential to follow specific dos and don'ts to ensure the process goes smoothly and errors are minimized. Here is a comprehensive list to guide you through filling out this form accurately.
By following these guidelines, you help to ensure that the claim process for supporting children through the Family and Children Funds is conducted efficiently and without unnecessary delay or error. Remember, accuracy is key in all areas of completing the State 28808 form.
There are several misconceptions about the State Form 28808, particularly regarding its purpose, the process of completing it, and its requirements. Clarifying these misconceptions ensures that individuals and organizations can accurately complete the form and comply with the regulations. Here are some of the common misconceptions:
Form is only for foster parents: This misconception arises because the form is often associated with foster care services. However, State Form 28808 is designed to be used by various vendors, including residential care providers, adoption services, and family preservation services, among others. It caters to a broad spectrum of child support services, not just those provided by foster parents.
Personal Social Security Numbers are widely required: While the form does ask for the last four digits of the Tax ID/SSN, it primarily requires this for individual providers like foster parents. This is a measure to protect personal information while ensuring the identification of the provider for processing payments.
Invoice number can be any length: There's a specific requirement that the invoice number must be no longer than 8 characters. This is often misunderstood, leading to the submission of forms with longer invoice numbers, which can cause processing delays.
Submission deadlines are flexible: The form clearly states that invoices must be received within 10 business days of the date of invoice. Some might think this deadline is flexible, however, adhering to this timeline is crucial for timely processing and payment.
Any ink color can be used for signatures: While the form can technically be signed with any ink, the instructions recommend using blue ink. This ensures that original documents can be easily distinguished from copies, a detail that's often overlooked.
All service types can be mixed on one invoice: One common mistake is including multiple service types on the same invoice. The form requires that only one overarching service type be selected for all service codes listed in the invoice, to simplify processing and auditing.
Service dates and claim period dates are interchangeable: The form distinguishes between the claim period—the month being billed—and the actual dates of service. Some providers confuse these two, leading to inaccurately completed forms. It's important to differentiate and accurately enter dates for each.
Rate adjustments or rebills can include new services: When submitting a rate adjustment or rebill due to denied past invoice lines, the perception might be that additional services can be added. However, these invoice types should only correct or appeal previously submitted information, not introduce new charges.
Submission guarantees payment: Submitting the form does not automatically guarantee payment. The form undergoes a review process, and discrepancies may necessitate additional verification or lead to denial. Providers must ensure that their submissions are accurate and complete to facilitate this process.
Understanding these nuances is crucial for providers seeking support for children through the Family and Children Funds. Accurate completion and submission of State Form 28808 help in the efficient processing of claims, ensuring that children receive the support and services they need.
When working with the State 28808 form, specifically designed for claiming support of children payable from Family and Children Funds in Indiana, understanding its various components and how to accurately complete it is crucial. Here are ten key takeaways to ensure that the process is both effective and compliant:
Following these guidelines will help ensure that submissions to the Indiana Department of Child Services via the State 28808 form are accurate and timely. This process not only facilitates the support of children in need but also ensures that vendors are properly compensated for their services within the scope of the law and the agreed contractual terms.
Land Contract Indiana Pdf - The contract includes a method for adjusting the monthly payment to cover tax and insurance costs accurately.
Indiana Form It-6 - Specifies the information needed from corporations to access their estimated tax payment history online.